
















 and acceptor (A) molecule which participate in FRET (Förster resonance energy transfer).")


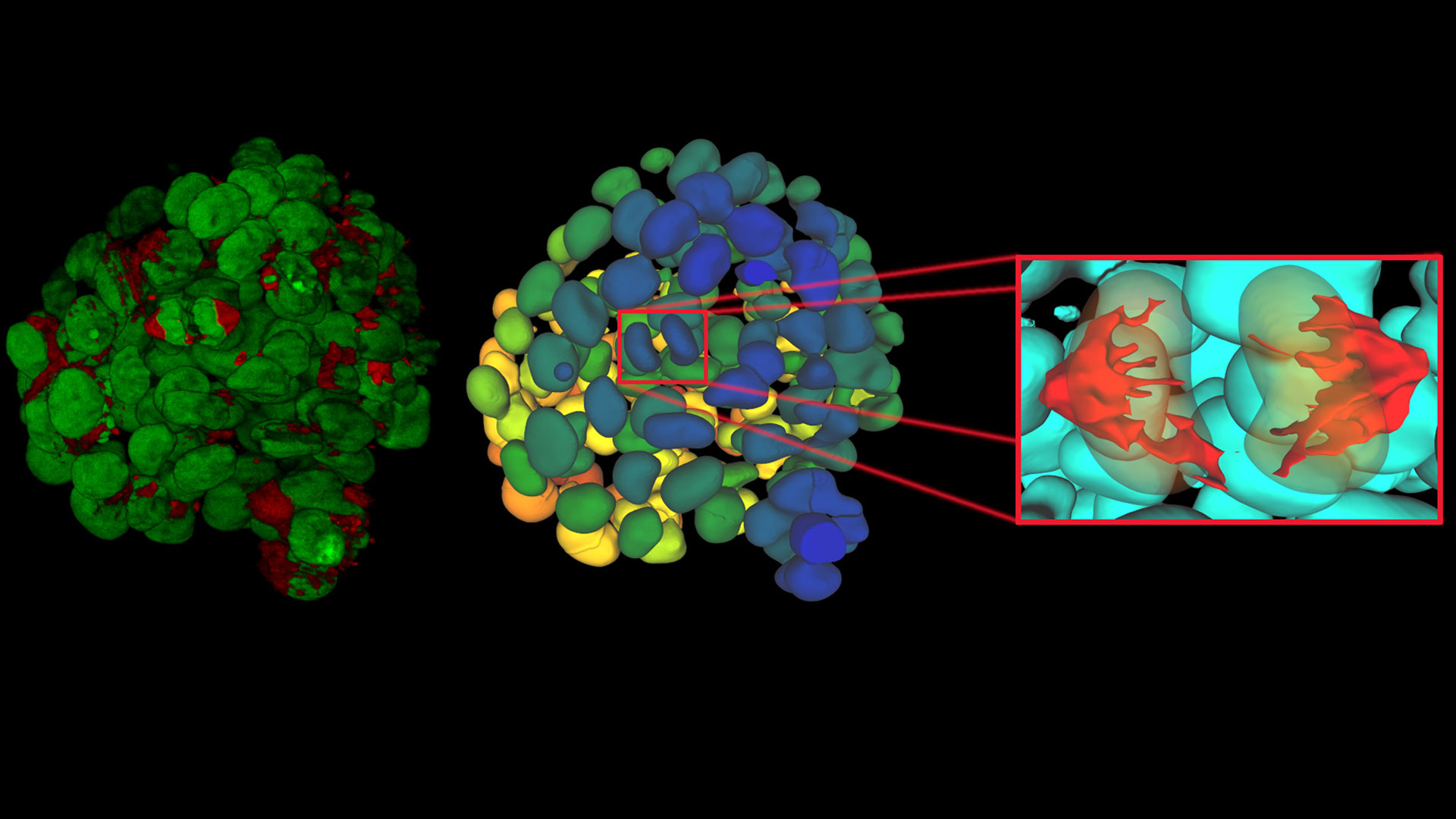
, insulin SGs (orange), microtubules (red), nucleus (yellow), and plasma membrane (transparent).")





The Viventis Deep light sheet microscope supports both live and cleared imaging on one configurable platform
Our Latest Articles
Spatial Proteomics Workflow in Blood Cancer (MPNs)
Megakaryocytes play a central role in the biology of myeloproliferative neoplasms (MPNs), yet their in vivo proteomic characterization remains a major challenge due to low abundance and disrupted…
Six Features to Consider when Choosing a Dental Microscope
The dental surgical microscope has become increasingly important for high-quality and successful dental medicine, particularly in the field of endodontics. A dentist can conduct micro-invasive…
Multiscale Imaging of Organoids: High Content to Light Sheet
Learn multiscale organoid imaging: fixed high content phenotyping, gentle dual view light sheet, and reproducible pipelines that turn 3D data into insights.
What is FRET with FLIM or as it is usually known FLIM-FRET?
Förster resonance energy transfer (FRET) is a well-established fluorescence-based technique which is used to study molecular interactions. It is useful for the analysis of protein-DNA and…
Ratiometric Imaging and Analysis of Ion Concentration in Cells
Many cellular functions depend on the dynamic balance of ions, electric potentials, and pH between the cytosol and surrounding extracellular space. Changes in these values affect cellular function.…
4 Key Benefits of 3D Digital Microscopy in Ophthalmic Surgery
3D digital visualization is rapidly transforming ophthalmic surgery. Modern 3D surgical microscopes enable surgeons to perform procedures using high-resolution digital displays rather than traditional…
High-Pressure Freezing Protocols for Ultrastructural 3D EM
High pressure freezing (HPF) can help preserve hydrated cells and tissues close to their biological state at the moment of immobilization, supporting more reliable ultrastructural interpretation than…
Ultramicrotome UC Enuity in Practice: Stable 15 nm Sections at ZFE
After using the UCT and UC6 ultramicrotomes, Claudia Mayrhofer calls UC Enuity a leap in stability—so robust that vibrations and temperature shifts don’t spoil sections, even with multiple users. Auto…
Ensuring Glass Quality with the Polarization Microscopy Advantage
Glass is one of the oldest materials known. Today, it is used for many applications, e.g., optical instruments, windows, doors, solar panels, containers for food, beverages, and medicine, so strict…
Expert Techniques for Superior Visualization in Cataract Surgery
Join renowned ophthalmic surgeons, Dr. Hussein Almuhtaseb and Mr. Simon Madge, as they share their clinical expertise and real-world surgical strategies during the 2025 Online Cataract Surgery…
ATTO-TEC Consumables
ATTO-TEC dyes have become a benchmark for fluorescence microscopy imaging, offering a highly differentiated panel. Their brightness and photostability make them the reagents of choice for demanding applications.

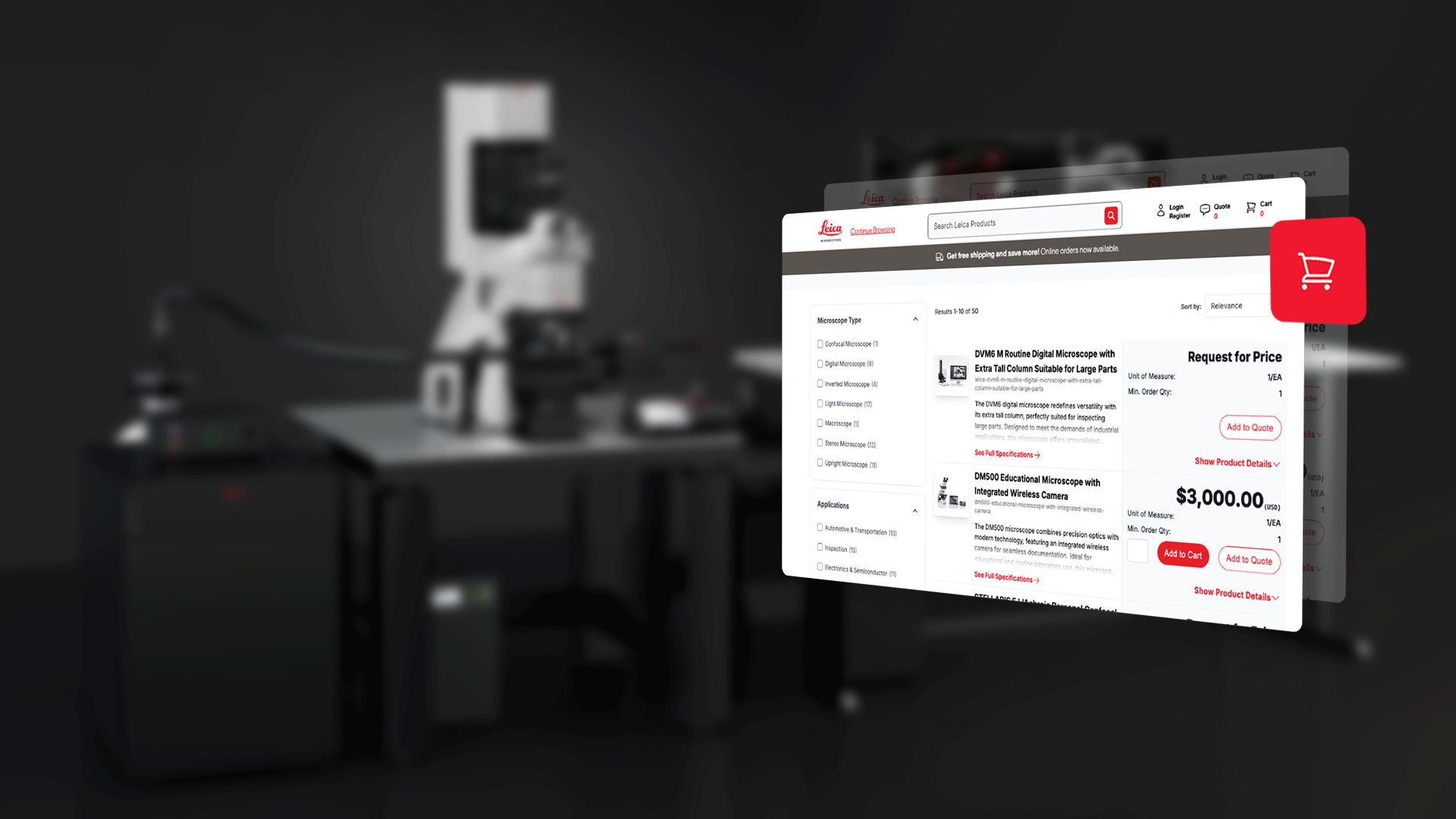
Customers gain access to microscopy solutions, software, and localized purchasing options in their local languages

The Launch Early Access Program (LEAP) from Leica Microsystems provides supported access to the ATTOAuriga reagent platform

Leica Microsystems launches the Viventis SCAPE light sheet microscope. It enables fast 3D light sheet imaging while using standard sample carriers.…

February 2026, Wetzlar, Germany - Leica Microsystems, a Danaher company and a leading provider of microscopy and scientific solutions, has appointed…
